
What is the origin of the Adalimumab?
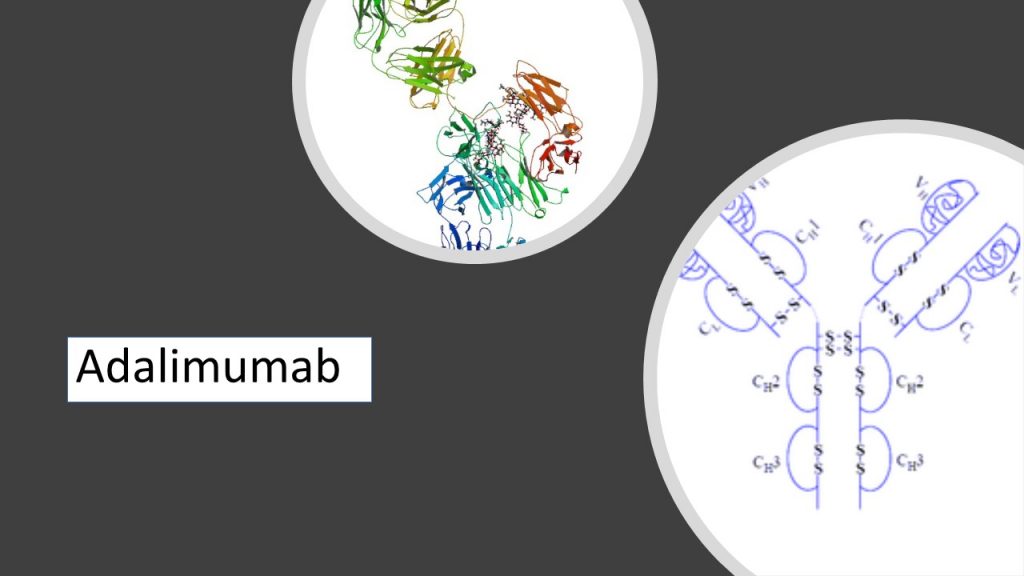
Adalimumab is a fully human IgG1 anti-TNF-α monoclonal antibody produced by phage display with a terminal half-life between 10 and 20 days. This antibody binds free and cell-bound TNF-α and blocks the binding with p55 and p75 receptors but does not interact with TNF-β. This antibody is used in pharmacy as a drug approved by WHO that induces cell lysis of TNF-expressing cells in the presence of complement.
How Adalimumab works?
According to the clinical tests Adalimumab reduces the signs and symptoms of severe rheumatoid arthritis. This therapeutic antibody inhibits radiographic damage, progression and improve physical function in moderate to severe RA that cannot be treated by the other disease-modifying anti-rheumatic drugs (DMARDs). It is also approved for treatment of Psoriatic arthritis, psoriasis, Crohn disease, and ulcerative colitis. The recommended dosage is an injection of 40 mg every other week. A few patients may require higher doses, for example 40 mg every week. The PREMIER early RA trial shows that the dose escalation was permitted for those not meeting American College of Rheumatology 20% improvement criteria (ACR20). Patients receiving adalimumab monotherapy need an increase to weekly dosing than those receiving combined adalimumab and Methotrexate (MTX) treatment (Adalimumab 25% – 11% Methotrexate). A single dose of adalimumab leads to significant and rapid clinical improvement, reduced acute-phase reactants, increased circulating lymphocyte levels, and significantly reduced systemic IL-6 and IL-1ra levels for 2 weeks. ACR20 response rates have varied from 46% to 73% in controlled dose-ranging monotherapy tests. A dose-dependent rise in ACR response rates was detected during a placebo-controlled monotherapy trial involving 544 patients with rheumatoid arthritis.
Which doses have positive effects on RA patients?
The ARMADA trial examined the effects of adalimumab on 271 patients with chronic disease. They have been treated unsuccessfully with Methotrexate. As a result of a 6-month multicenter trial, patients continued to receive stable doses of MTX (mean, 16 to 17 mg/wk) combined with adalimumab in doses of 20 mg, 40 mg, or 80 mg of adalimumab every 2 weeks. ACR20 response rates were 14%, 48%, 66%, and 66% for those taking placebo, 20 mg adalimumab, 40 mg adalimumab, and 80 mg adalimumab, respectively. Other tests showed the positive effect and radiographic outcomes in a 52-week trial in 619 patients. Adalimumab in doses of 20 mg or 40 mg every other week or placebo were given to MTX partial responders and ACR20 response rates after 52 weeks were 24%, 55%, and 59% in the placebo, 20 mg adalimumab, and 40 mg adalimumab groups. Reactions to this treatment was permanent in the 457 patients who received long-term open-label adalimumab.
The PREMIER trial established the positive effects of adalimumab therapy during the early stage of rheumatoid arthritis RA. During a 2-year trial, DMARD-naive patients received either adalimumab, MTX, or the combination of MTX and adalimumab. There were no differences between Adalimumab and MTX monotherapy but the combination of both drug results in a significantly better response.
Major clinical response rates were 2-fold higher with MTX combined with adalimumab than in the cases of adalimumab monotherapy.